|
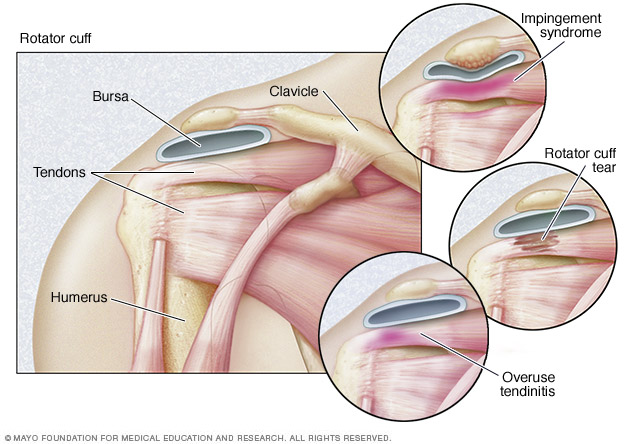
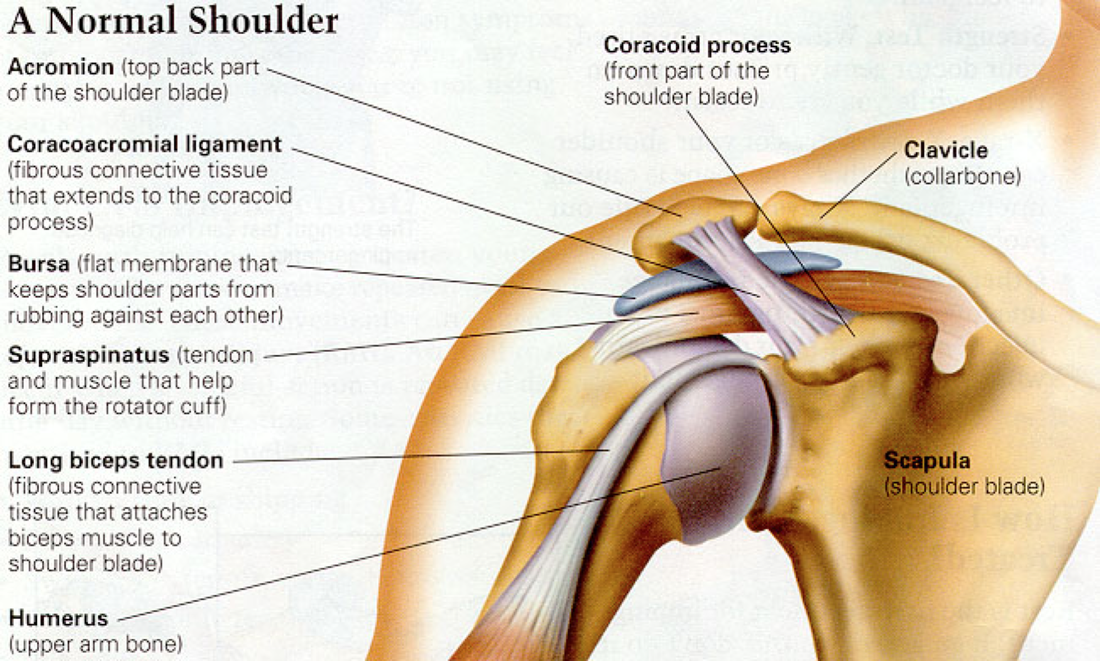
The rotator cuff is made up of four muscles: supraspinatus (on top), subscapularis (in front), and infraspinatus and teres minor (in back). All four of the muscles originate on the scapula (shoulder blade) and attach to the humerus (upper arm bone). The principle function of the rotator cuff is to stabilize and center the humerus in the shoulder socket while the bigger muscles of the shoulder such as the deltoids move the arm. As the name suggests, the rotator cuff plays a large role in internal and external rotation of the arm. When the rotator cuff gets damaged and this delicate muscular balance in the shoulder is disrupted, it can have major effects on the function of the arm.
|
|
Kenova
|
Barboursville
|
Milton
|
HUNTINGTON
|



