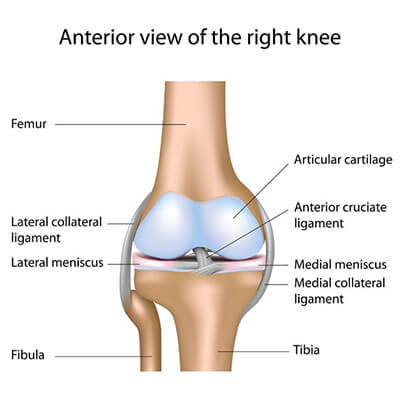
Anatomy of the KneeThe knee is the largest joint in the human body and a common source of athletic-related injuries. Classified as a pivotal hinge joint, the knee allows for straightening and bending in one direction, with some twisting (screw home mechanism). The knee joint is made up of bones, cartilage, ligaments, tendons, bursae, and meniscus. A injury to any one of these structures can cause knee pain.
|
|
Kenova
|
Barboursville
|
Milton
|
HUNTINGTON
|



